Thursday, November 03, 2011
RISKS in various Keratoconus Treatments.
A while back a person called Emu left the following comment and questions:
"Thanks! I've found this a very interesting blog. Are there any known risks relating to C3-R treatment? This may be available elsewhere but I have been unable to find statistics on the success of transplants, and statistics on how successful (% that still need contacts, that only need glasses etc).
I suspect that this is something that other keratoconus patients would be interested in. Perhaps you would consider posting on this at some stage?"
Unfortunately irrespective of whatever treatment is attempted with any disease, there are always risks of something going wrong. Keratoconus is no different.
The first question that Emu asks is about risks with C3-R or Collagen Cross-Linking. This procedure as you might have already read is great at slowing down further progression but:
Using the Australian Corneal Graft Registry as a reference we can say that 50% of corneal grafts will fail by the 15 year point. The other 50% will slowly fail one by one as the years progress. The oldest corneal graft I have seen was gentleman that was referred for a scleral lens fitting. the graft was 45 years old and is still functioning at the moment with the contact lens - he passes a drivers license test - amazing!
I would say that eventually every patient that has had a corneal transplant will benefit from glasses. How many will require contact lenses is more difficult to answer. Eventually it is not unreasonable to say that up to 50% will require specialized contact lenses to see to a satisfactory level.
"Thanks! I've found this a very interesting blog. Are there any known risks relating to C3-R treatment? This may be available elsewhere but I have been unable to find statistics on the success of transplants, and statistics on how successful (% that still need contacts, that only need glasses etc).
I suspect that this is something that other keratoconus patients would be interested in. Perhaps you would consider posting on this at some stage?"
Unfortunately irrespective of whatever treatment is attempted with any disease, there are always risks of something going wrong. Keratoconus is no different.
The first question that Emu asks is about risks with C3-R or Collagen Cross-Linking. This procedure as you might have already read is great at slowing down further progression but:
- There is a small risk of an infection for approximately 4 - 5 days after the procedure as the cornea is healing.
- There is a risk of significant corneal scarring.
- There is a risk of decompensation of the cornea, but this might occur because the procedure was attempted on a cornea that was too thin.
- All these risks are rare but they need to be revealed before a person makes the decision to go ahead.
Using the Australian Corneal Graft Registry as a reference we can say that 50% of corneal grafts will fail by the 15 year point. The other 50% will slowly fail one by one as the years progress. The oldest corneal graft I have seen was gentleman that was referred for a scleral lens fitting. the graft was 45 years old and is still functioning at the moment with the contact lens - he passes a drivers license test - amazing!
I would say that eventually every patient that has had a corneal transplant will benefit from glasses. How many will require contact lenses is more difficult to answer. Eventually it is not unreasonable to say that up to 50% will require specialized contact lenses to see to a satisfactory level.
Thursday, October 27, 2011
KERATOCONUS UPDATE: I have been away for a while
Hi it's Dr Jim Kokkinakis finally back again. I have been really busy seeing patients with keratoconus and computer vision induced eye strain.
I must apologise for forgetting about this blog, but I have also been overwhelmed with inquiries from all over the world about keratoconus. It really is a very frustrating condition. The stories keep coming through and invariably nearly all cases that are frustrated are caused by inaccurate information or treatment.
I have written the following to help out patients with keratoconus:
Remember as we have said before: Keratoconus is not a blinding eye condition, it is a big inconvenience. Managed appropriately your life can return to being normal.
I must apologise for forgetting about this blog, but I have also been overwhelmed with inquiries from all over the world about keratoconus. It really is a very frustrating condition. The stories keep coming through and invariably nearly all cases that are frustrated are caused by inaccurate information or treatment.
I have written the following to help out patients with keratoconus:
- "7 Vital Facts you need to know about Keratoconus...but Don't". You can find this very simple and short document on The Eye Practice website. CLICK HERE. Believe it or not it has been downloaded over 15,000 times from around the world.
- I have started a general eye care blog, which not only talks about Keratoconus, but all sorts of important eye information. It also can be found on The Eye Practice website. CLICK HERE.
- With 3 other prominent keratoconus specialists from Sydney and Melbourne, we have collaborated to write a book on keratoconus. This is likely to be in print before the end of the year. As far as we know nothing like this has been written for the layperson before. If you would like to be notified when it is published register your interest by emailing me at: jimkokkinakis@gmail.com
- I have set up the website: www.keratoconus.com.au
Remember as we have said before: Keratoconus is not a blinding eye condition, it is a big inconvenience. Managed appropriately your life can return to being normal.
Monday, May 08, 2006
More on Riboflavin treatment
Eye treatment could replace surgery
From: AAP
By Jane BunceApril 16, 2006
A SIMPLE treatment using Vitamin B2 and ultraviolet light could replace major corneal transplant surgery for Australian patients in a revolutionary eye treatment trial.Scientists believe the procedure will save the eyesight of up to 50,000 Australians with the degenerative eye disease keratoconus.
Keratoconus sufferers experience a progressive cone-like distortion of the normally round-shaped cornea, which can initially be corrected with glasses or contact lenses but can lead to blindness and the need for a corneal transplant.
But the new treatment can stop the disease by strengthening the cornea to prevent it changing shape.
German doctor Christin Wittig is in Australia to complete the randomised trial involving 100 patients at Melbourne's Royal Victorian Eye and Ear Hospital over the next year.
Dr Wittig said about 250 patients had undergone the procedure in Germany in the past five years.
It had stopped the progression of the disease in all, and none had suffered serious complications.
"It treats the cause of the disease, not just the symptoms, and stops patients undergoing major surgery, so it's a pretty big step forward really," Dr Wittig said.
She said it was most effective in the early stages of the disease because it could not reverse the deterioration of the cornea.
The treatment involves scraping a layer of skin off the patient's eye, applying Vitamin B2, also called riboflavin, using an eye dropper and exposing the cornea to a measured dose of UVA light.
The light activates the B2 to produce oxygen radicals, which begin a chemical reaction that binds and cross-links collagen fibres in the cornea and thereby strengthen it, Dr Wittig said.
She said the procedure had much less impact on patients' lives than a corneal transplant, was cheaper and quicker and could easily be taken to regional areas.
A single transplant costs around $3000, while the new treatment costs about $2500 for the equipment and about $1000 for riboflavin to treat 60 patients.
Melbourne travel agent Tanya Wilkinson, 26, who has suffered keratoconus since she was 10, had a corneal transplant in her left eye in 2001.
The disease still affects Mrs Wilkinson's right eye, and she could need a second transplant within seven years.
She said she preferred the new procedure because a transplant required 18 months of post-operative care and could be rejected.
"It's a great prospect," she said.
Corneal Unit head Dr Grant Snibson said if the trial appeared successful after six months, and the hospital received ethics committee approval, it would offer the procedure to other patients.
Keratoconus is estimated to occur in one in every 400 to 2000 Australians and usually begins between the ages of eight and 45.
More than 1200 corneal transplants are performed in Australia every year.
We have been inundated with phone enquiries about this promising treatment.
Currently approximately 20% of patients with clinically significant keratoconus will require corneal transplantation. This treatment is still in its infancy but it could be the first line of treatment as soon a diagnosis of keratoconus is made. As long as there are no long term side effects it could be at its most powerful between the ages of 15 - 25 when keratoconus is most likely to progress.
Stay tuned as The Eye Practice is in constant communication with the leading corneal surgeons. We promise that we will keep constantly up to date with the latest advancements in keratoconus.
Visit our website: www.theeyepractice.com.au for more information about keratoconus and other eye issues.
From: AAP
By Jane BunceApril 16, 2006
A SIMPLE treatment using Vitamin B2 and ultraviolet light could replace major corneal transplant surgery for Australian patients in a revolutionary eye treatment trial.Scientists believe the procedure will save the eyesight of up to 50,000 Australians with the degenerative eye disease keratoconus.
Keratoconus sufferers experience a progressive cone-like distortion of the normally round-shaped cornea, which can initially be corrected with glasses or contact lenses but can lead to blindness and the need for a corneal transplant.
But the new treatment can stop the disease by strengthening the cornea to prevent it changing shape.
German doctor Christin Wittig is in Australia to complete the randomised trial involving 100 patients at Melbourne's Royal Victorian Eye and Ear Hospital over the next year.
Dr Wittig said about 250 patients had undergone the procedure in Germany in the past five years.
It had stopped the progression of the disease in all, and none had suffered serious complications.
"It treats the cause of the disease, not just the symptoms, and stops patients undergoing major surgery, so it's a pretty big step forward really," Dr Wittig said.
She said it was most effective in the early stages of the disease because it could not reverse the deterioration of the cornea.
The treatment involves scraping a layer of skin off the patient's eye, applying Vitamin B2, also called riboflavin, using an eye dropper and exposing the cornea to a measured dose of UVA light.
The light activates the B2 to produce oxygen radicals, which begin a chemical reaction that binds and cross-links collagen fibres in the cornea and thereby strengthen it, Dr Wittig said.
She said the procedure had much less impact on patients' lives than a corneal transplant, was cheaper and quicker and could easily be taken to regional areas.
A single transplant costs around $3000, while the new treatment costs about $2500 for the equipment and about $1000 for riboflavin to treat 60 patients.
Melbourne travel agent Tanya Wilkinson, 26, who has suffered keratoconus since she was 10, had a corneal transplant in her left eye in 2001.
The disease still affects Mrs Wilkinson's right eye, and she could need a second transplant within seven years.
She said she preferred the new procedure because a transplant required 18 months of post-operative care and could be rejected.
"It's a great prospect," she said.
Corneal Unit head Dr Grant Snibson said if the trial appeared successful after six months, and the hospital received ethics committee approval, it would offer the procedure to other patients.
Keratoconus is estimated to occur in one in every 400 to 2000 Australians and usually begins between the ages of eight and 45.
More than 1200 corneal transplants are performed in Australia every year.
We have been inundated with phone enquiries about this promising treatment.
Currently approximately 20% of patients with clinically significant keratoconus will require corneal transplantation. This treatment is still in its infancy but it could be the first line of treatment as soon a diagnosis of keratoconus is made. As long as there are no long term side effects it could be at its most powerful between the ages of 15 - 25 when keratoconus is most likely to progress.
Stay tuned as The Eye Practice is in constant communication with the leading corneal surgeons. We promise that we will keep constantly up to date with the latest advancements in keratoconus.
Visit our website: www.theeyepractice.com.au for more information about keratoconus and other eye issues.
Wednesday, March 08, 2006
Riboflavin Treatment for Keratoconus
Rather than describe the procedure myself I will quote the following article from USAEyes.org
"Keratoconus is a disease of the cornea that makes the cornea become weak and may gradually bulge outward. Most often, this bulging is in the lower half of the cornea and first presents as astigmatism, however not all astigmatism is due to keratoconus. In mild or early stages of keratoconus (forme fruste keratoconus), eyeglasses may correct the astigmatic vision.
The abnormal curvature of the cornea due to keratoconus changes the cornea’s refractive error producing moderate to severe blurriness of vision. As keratoconus advances, rigid gas-permeable (RGP) contact lenses maybe the only non-surgical way to achieve clear vision. If keratoconus continues to advance, scarring of the central cornea may occur.
Approximately half of keratoconus patients have no negative lifestyle effects beyond corrective lenses. The cornea stabilizes after a few years without ever causing severe vision problems. For others, the only resolution to keratoconus has been PKP, with a long healing period and unpredictable refractive error. Even after corneal transplant PKP, keratoconus can reoccur in the new donor cornea. Fortunately, there are two new methods to treat keratoconus that are much less invasive than a corneal transplant.
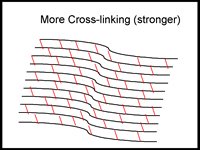
One new keratoconus treatment is C3-R (Corneal Collagen Crosslinking with Riboflavin) that has been proven to strengthen the weak corneal structure. This method works by increasing collagen crosslinking, which are the natural "anchors" within the cornea. These anchors are responsible for preventing the cornea from bulging out and becoming steep and irregular, consequence of advanced keratoconus.
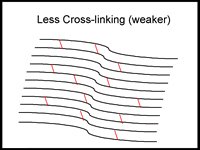


The 30-minute C3-R treatment is performed in the doctor's office. During the treatment, custom-made riboflavin eye drops are applied to the cornea, which is then activated by ultraviolet light. This amazingly simple process has been shown in laboratory and clinical studies to increase the amount of collagen cross-linking in the cornea and strengthen the cornea. In published European studies, such treatments were proven safe and effective in patients.
Another new treatment for keratoconus is Intacs. Intacs are a medical device approved by the FDA for the correction of 1.00 to 3.00 diopters of myopia (nearsighted, shortsighted) and virtually no astigmatism. Intacs inserts are the only refractive surgery procedure that adds structural integrity to the cornea. This unique attribute made Intacs an ideal treatment for keratoconus.
Intacs are clear small semicircular plastic rings of various thickness that are inserted within the cornea at its outer edges. Insertion of these rings flatten the central area of the cornea and correct myopic refractive error. A major advantage of Intacs is that no tissue is removed and there is no ablation or incision across the visual axis.
Intacs surgery is not truly reversible because of the incision, but the Intacs can be completely removed or exchanged for a different size. Intacs inserts cannot be felt by the patient and are no more visible than a contact lens. After insertion and healing, Intacs require no maintenance.
The placement of Intacs inserts remodels and reinforces the cornea, eliminating some or all of the irregularities caused by keratoconus. Follow-up visits will be required to monitor the healing process and to evaluate the visual benefits of the procedure. Even after a successful Intacs procedure for keratoconus, glasses or contacts may be required, however Intacs have been shown to improve vision and reduce or stop the progression of keratoconus, thereby saving the patient from needing PKP.
Intacs have been approved for the treatment of keratoconus by the FDA under a Humanitarian Device Exemption (HDE) Humanitarian Use Devices (HUDs) are medical devices specially designated by the FDA for use in the treatment of fewer than 4000 patients per year with rare medical conditions.
C3-R treatments can be combined with Intacs to flatten the keratoconus cone even more than with Intacs alone. In these cases, C3-R treatments stabilize keratoconus from getting worse as well as help the Intacs reverse the keratoconus steepening that had already occurred."
From what I can see so far this is an exciting development. If the progression can be stopped or even significantly reduced, it will mean that many more keratoconic patients will be able to wear glasses and / or will need less contact lens changes. You will also notice that Intacs have again been mentioned. This is indeed some great stuff. Stay tuned and I hope to post more in the near future. Click to visit my web site for more information about keratoconus
"Keratoconus is a disease of the cornea that makes the cornea become weak and may gradually bulge outward. Most often, this bulging is in the lower half of the cornea and first presents as astigmatism, however not all astigmatism is due to keratoconus. In mild or early stages of keratoconus (forme fruste keratoconus), eyeglasses may correct the astigmatic vision.
The abnormal curvature of the cornea due to keratoconus changes the cornea’s refractive error producing moderate to severe blurriness of vision. As keratoconus advances, rigid gas-permeable (RGP) contact lenses maybe the only non-surgical way to achieve clear vision. If keratoconus continues to advance, scarring of the central cornea may occur.
Approximately half of keratoconus patients have no negative lifestyle effects beyond corrective lenses. The cornea stabilizes after a few years without ever causing severe vision problems. For others, the only resolution to keratoconus has been PKP, with a long healing period and unpredictable refractive error. Even after corneal transplant PKP, keratoconus can reoccur in the new donor cornea. Fortunately, there are two new methods to treat keratoconus that are much less invasive than a corneal transplant.
One new keratoconus treatment is C3-R (Corneal Collagen Crosslinking with Riboflavin) that has been proven to strengthen the weak corneal structure. This method works by increasing collagen crosslinking, which are the natural "anchors" within the cornea. These anchors are responsible for preventing the cornea from bulging out and becoming steep and irregular, consequence of advanced keratoconus.


The 30-minute C3-R treatment is performed in the doctor's office. During the treatment, custom-made riboflavin eye drops are applied to the cornea, which is then activated by ultraviolet light. This amazingly simple process has been shown in laboratory and clinical studies to increase the amount of collagen cross-linking in the cornea and strengthen the cornea. In published European studies, such treatments were proven safe and effective in patients.
Another new treatment for keratoconus is Intacs. Intacs are a medical device approved by the FDA for the correction of 1.00 to 3.00 diopters of myopia (nearsighted, shortsighted) and virtually no astigmatism. Intacs inserts are the only refractive surgery procedure that adds structural integrity to the cornea. This unique attribute made Intacs an ideal treatment for keratoconus.
Intacs are clear small semicircular plastic rings of various thickness that are inserted within the cornea at its outer edges. Insertion of these rings flatten the central area of the cornea and correct myopic refractive error. A major advantage of Intacs is that no tissue is removed and there is no ablation or incision across the visual axis.
Intacs surgery is not truly reversible because of the incision, but the Intacs can be completely removed or exchanged for a different size. Intacs inserts cannot be felt by the patient and are no more visible than a contact lens. After insertion and healing, Intacs require no maintenance.
The placement of Intacs inserts remodels and reinforces the cornea, eliminating some or all of the irregularities caused by keratoconus. Follow-up visits will be required to monitor the healing process and to evaluate the visual benefits of the procedure. Even after a successful Intacs procedure for keratoconus, glasses or contacts may be required, however Intacs have been shown to improve vision and reduce or stop the progression of keratoconus, thereby saving the patient from needing PKP.
Intacs have been approved for the treatment of keratoconus by the FDA under a Humanitarian Device Exemption (HDE) Humanitarian Use Devices (HUDs) are medical devices specially designated by the FDA for use in the treatment of fewer than 4000 patients per year with rare medical conditions.
C3-R treatments can be combined with Intacs to flatten the keratoconus cone even more than with Intacs alone. In these cases, C3-R treatments stabilize keratoconus from getting worse as well as help the Intacs reverse the keratoconus steepening that had already occurred."
From what I can see so far this is an exciting development. If the progression can be stopped or even significantly reduced, it will mean that many more keratoconic patients will be able to wear glasses and / or will need less contact lens changes. You will also notice that Intacs have again been mentioned. This is indeed some great stuff. Stay tuned and I hope to post more in the near future. Click to visit my web site for more information about keratoconus
Tuesday, February 21, 2006
A Common Keratoconus Story
The following is an article from a paper in the US:
Posted February 20, 2006
Threat of blindness leads ex-Packer to benefit
Blaise Winter knows his future may hold a cornea transplant and the former Packers defensive lineman says he is scared to death.
Winter, who will speak at a Prevent Blindness benefit Friday, was diagnosed with keratoconus more than 10 years ago. Keratoconus is a noninflammatory eye condition in which the normally round dome-shaped cornea progressively thins causing a cone-like bulge to develop. This results in significant visual impairment, according to the National Keratoconus Foundation.
"The cornea is the clear window of the eye and is responsible for refracting most of the light coming into the eye. Therefore, abnormalities of the cornea severely affect the way we see the world making simple tasks, like driving, watching TV or reading a book difficult," according to the foundation.
Glasses and soft contact lenses may be used to correct the mild nearsightedness and astigmatism that is caused in the early stages of keratoconus. As the disorder progresses and the cornea continues to thin and change shape, rigid gas-permeable contact lenses can be prescribed to correct the vision. In severe cases, a corneal transplant may be needed because of scarring, extreme thinning or contact-lens intolerance.
Winter said he first noticed problems when he was in high school. "I fought wearing glasses, and I never wore them for games. I was really excited when I was fitted with contacts." He comfortably wore the soft lenses as an athlete.
After a few years, the comfort faded, and he finally was diagnosed with keratoconus. "The only way to get a comfort level and address the problem was to get into hard lenses," he said.
At 44, he is aware that there is "always the outside worry that they can't force the eye into the right shape with glasses or contacts and I'll be in trouble. If I don't wear contacts, I'll walk into a wall or a door. I can't see my wife's face if she's two feet in front of me.
"I'm scared to death about this. I think no matter how often the cornea transplant procedure is done, I still don't want to hear a doctor say I'll need one."
His eyes have developed ulcers in the corners from wearing contacts so much, he said. "I wear contacts for 14 to 17 hours a day. It hurts, but I can't get home without them."
"I have two little boys. I want to see them — not just hear them or feel them — grow up. I want to continue to do my motivational work," Winter said. He is a motivational speaker living in Appleton.
Because it's not an ailment that people can see, he suffers privately with it. "I was born with a cleft palate. People can see my scar; my speech is a little different. But, people don't see eye problems.
"We have a tendency to take our vision for granted. It's tough to deal with. No one gives you sympathy. When I drop a contact on the floor, I panic. I can't see to find it. I always have to carry a spare set."
Winter is committed to Prevent Blindness on both the local and national levels.
"There are a lot of types of vision problems," he said. "People are suffering. I'm committed to getting people aware of different types of vision problems."
The fear of going blind of keratoconus is a huge issue for many of my patients. The issue lies in the fact that a keratoconic patient feels like they are always on a treadmill. Apart from regular eye exams sometimes every three months, the fear of losing lenses and of the lenses no longer fitting and being forced to do a corneal transplant is constantly on their minds. The best way to cope with this ongoing activity is to just accept it and trust that the practitioner treating them will always keep their interest at heart. Finding a practitioner that understands the issues associated with keratoconus is a matter of finding someone that sees many keratoconic patients.
Every keratoconic patient is unique in their own way, but if time is spent analysing the problems that come up, the overwhelming majority of problems have very satisfactory solutions.
If you are not seeing a keratoconic specialist just ask! You will find that most practitioners will only be too willing to help you find someone that can help you.
Posted February 20, 2006
Threat of blindness leads ex-Packer to benefit
Blaise Winter knows his future may hold a cornea transplant and the former Packers defensive lineman says he is scared to death.
Winter, who will speak at a Prevent Blindness benefit Friday, was diagnosed with keratoconus more than 10 years ago. Keratoconus is a noninflammatory eye condition in which the normally round dome-shaped cornea progressively thins causing a cone-like bulge to develop. This results in significant visual impairment, according to the National Keratoconus Foundation.
"The cornea is the clear window of the eye and is responsible for refracting most of the light coming into the eye. Therefore, abnormalities of the cornea severely affect the way we see the world making simple tasks, like driving, watching TV or reading a book difficult," according to the foundation.
Glasses and soft contact lenses may be used to correct the mild nearsightedness and astigmatism that is caused in the early stages of keratoconus. As the disorder progresses and the cornea continues to thin and change shape, rigid gas-permeable contact lenses can be prescribed to correct the vision. In severe cases, a corneal transplant may be needed because of scarring, extreme thinning or contact-lens intolerance.
Winter said he first noticed problems when he was in high school. "I fought wearing glasses, and I never wore them for games. I was really excited when I was fitted with contacts." He comfortably wore the soft lenses as an athlete.
After a few years, the comfort faded, and he finally was diagnosed with keratoconus. "The only way to get a comfort level and address the problem was to get into hard lenses," he said.
At 44, he is aware that there is "always the outside worry that they can't force the eye into the right shape with glasses or contacts and I'll be in trouble. If I don't wear contacts, I'll walk into a wall or a door. I can't see my wife's face if she's two feet in front of me.
"I'm scared to death about this. I think no matter how often the cornea transplant procedure is done, I still don't want to hear a doctor say I'll need one."
His eyes have developed ulcers in the corners from wearing contacts so much, he said. "I wear contacts for 14 to 17 hours a day. It hurts, but I can't get home without them."
"I have two little boys. I want to see them — not just hear them or feel them — grow up. I want to continue to do my motivational work," Winter said. He is a motivational speaker living in Appleton.
Because it's not an ailment that people can see, he suffers privately with it. "I was born with a cleft palate. People can see my scar; my speech is a little different. But, people don't see eye problems.
"We have a tendency to take our vision for granted. It's tough to deal with. No one gives you sympathy. When I drop a contact on the floor, I panic. I can't see to find it. I always have to carry a spare set."
Winter is committed to Prevent Blindness on both the local and national levels.
"There are a lot of types of vision problems," he said. "People are suffering. I'm committed to getting people aware of different types of vision problems."
The fear of going blind of keratoconus is a huge issue for many of my patients. The issue lies in the fact that a keratoconic patient feels like they are always on a treadmill. Apart from regular eye exams sometimes every three months, the fear of losing lenses and of the lenses no longer fitting and being forced to do a corneal transplant is constantly on their minds. The best way to cope with this ongoing activity is to just accept it and trust that the practitioner treating them will always keep their interest at heart. Finding a practitioner that understands the issues associated with keratoconus is a matter of finding someone that sees many keratoconic patients.
Every keratoconic patient is unique in their own way, but if time is spent analysing the problems that come up, the overwhelming majority of problems have very satisfactory solutions.
If you are not seeing a keratoconic specialist just ask! You will find that most practitioners will only be too willing to help you find someone that can help you.
Friday, February 17, 2006
Corneal Transplantation for Keratoconus
A corneal transplant has been the mainstay of treatment for keratoconus if contact lenses fail due to discomfort or unsatisfactory visual quality. I found an interesting article a few days ago about an anaesthetist in the UK, who finally decided to have a corneal transplant at 50.
Follow the link to the Evening Times newspaper that is published in the UK and read the story. It brings up some interesting points that are worth discussing.
http://www.eveningtimes.co.uk/hi/news/5049013.html
Today another article about a minister of the church in Scotland, who allowed himself to go blind because:
"I waited until I had nothing to lose and everything to gain." The article follows:
I was blind . . now i can see
A BLIND minister has said an emotional thank you to the family who gave him his sight back. Port Glasgow man Andrew MacLean suffers from a rare eye condition which left him in need of a cornea transplant. Almost two years after undergoing surgery, the St Andrew's minister was able to see. New laws have been pushed through parliament to increase the number of organ donors in Scotland. Reverend MacLean said: "I want to thank the family of my donor. "If someone has just lost a loved one tragically in an accident it is an amazing gesture to give someone else the gift, in my case of my sight, and for others the gift of life." In September last year Reverend MacLean had vision out of his right eye for the first time in over three years. Nearly two years before he had undergone the surgery to give him sight. Andrew will need another transplant in the future to give him vision in his left eye. The father-of-two, who spent most of his life wearing contact lenses to correct his condition known as keratoconus which in extreme cases like Andrew's can make you go blind. He admitted delaying surgery until his vision was gone completely because he was scared to go ahead with a transplant. Andrew added: "I waited until I had nothing to lose and everything to gain." The surgery has given him a new hunger for life. Mr MacLean said: "I still can't believe it. I look out and appreciate what an extraordinary, beautiful world we live in. Before I lost my sight I didn't realise just how beautiful it was." Although he is over the moon to be able to see a whole new world, Mr MacLean says he does not regret for one minute being blind. He said: "I do not regret having a disability. People are enormously kind. When I was waiting for a bus I used to stop drivers to ask them where they were going. I didn't always have a stick but they were always great with me." Mr MacLean also recalls a group of football fans taking time out from celebrating a victory for their team to help him down a hill. Earlier this month a new bill was introduced that means relatives of a registered organ donor will no longer have the right to veto the person's wishes.
This story appeared in the Greenock Telegraph on Sat, 18 Feb, 2006
These sorts of cases really do not need to happen, even here in NSW where corneal transplant tissue is difficult to come by. Once contact lenses have failed (and this only occurs in about 5% of cases) the contact lens specialist normally has a good relationship with a number of expert corneal transplant surgeons and therefore a prompt transpant normally can be promptly organised. Remember corneal transplants very rarely fail.
Follow the link to the Evening Times newspaper that is published in the UK and read the story. It brings up some interesting points that are worth discussing.
http://www.eveningtimes.co.uk/hi/news/5049013.html
Today another article about a minister of the church in Scotland, who allowed himself to go blind because:
"I waited until I had nothing to lose and everything to gain." The article follows:
I was blind . . now i can see
A BLIND minister has said an emotional thank you to the family who gave him his sight back. Port Glasgow man Andrew MacLean suffers from a rare eye condition which left him in need of a cornea transplant. Almost two years after undergoing surgery, the St Andrew's minister was able to see. New laws have been pushed through parliament to increase the number of organ donors in Scotland. Reverend MacLean said: "I want to thank the family of my donor. "If someone has just lost a loved one tragically in an accident it is an amazing gesture to give someone else the gift, in my case of my sight, and for others the gift of life." In September last year Reverend MacLean had vision out of his right eye for the first time in over three years. Nearly two years before he had undergone the surgery to give him sight. Andrew will need another transplant in the future to give him vision in his left eye. The father-of-two, who spent most of his life wearing contact lenses to correct his condition known as keratoconus which in extreme cases like Andrew's can make you go blind. He admitted delaying surgery until his vision was gone completely because he was scared to go ahead with a transplant. Andrew added: "I waited until I had nothing to lose and everything to gain." The surgery has given him a new hunger for life. Mr MacLean said: "I still can't believe it. I look out and appreciate what an extraordinary, beautiful world we live in. Before I lost my sight I didn't realise just how beautiful it was." Although he is over the moon to be able to see a whole new world, Mr MacLean says he does not regret for one minute being blind. He said: "I do not regret having a disability. People are enormously kind. When I was waiting for a bus I used to stop drivers to ask them where they were going. I didn't always have a stick but they were always great with me." Mr MacLean also recalls a group of football fans taking time out from celebrating a victory for their team to help him down a hill. Earlier this month a new bill was introduced that means relatives of a registered organ donor will no longer have the right to veto the person's wishes.
This story appeared in the Greenock Telegraph on Sat, 18 Feb, 2006
These sorts of cases really do not need to happen, even here in NSW where corneal transplant tissue is difficult to come by. Once contact lenses have failed (and this only occurs in about 5% of cases) the contact lens specialist normally has a good relationship with a number of expert corneal transplant surgeons and therefore a prompt transpant normally can be promptly organised. Remember corneal transplants very rarely fail.


Thursday, February 16, 2006
Intacs
Yesterday I had a patient that enquired about a relatively new procedure called "Intacs" for keratoconus. Today I see the following article:
"Cutting hair for a worthy cause
Moxie hairdresser sets up fundraisers for a friend in need
By John C. Ensslin, Rocky Mountain News February 13, 2006
Erynn Simone looked across the room at Moxie Hair Co. in Denver, where a few feet away Talie Ayers, one of her childhood friends, was straightening a young woman's jet-black hair.
Simone, 22, could not see Ayers, nor the young woman.
That was why Ayers and six other hair stylists were working on a Sunday when the Capitol Hill hair salon normally would have been closed.
Simone is gradually losing her eyesight to keratoconus, an eye condition in which the normally dome- shaped cornea thins, causing a cone-like bulge of the cornea and blurred vision.
On Friday, Simone is scheduled to undergo a procedure to correct the condition. She will receive Intacs, which according to the National Keratoconus Foundation's Web site, are trademark prescription inserts approved by the Food and Drug Administration in July 2004.
Intacs are micro-thin, semi-circular plastic rings that are inserted into the mid-layer of the cornea, in an attempt to flatten it and improve vision.
The relatively new procedure will cost Simone about $7,000 and it is not approved by her medical insurance. So on Sunday, the hair stylists set to work, hoping to raise as much as they can toward the cost.
"Without the fundraiser, I probably wouldn't have the option of doing it. There's no way I would have the money," said Simone, who teaches environmental education in an after-school program at the Wild Bear Center for Nature Discovery in Nederland.
Ayers, who grew up with Simone in Three Rivers, Mich., had to convince her friend to let the hair salon do the fundraiser.
"I've just known her for so long," Ayers said. "If I could do anything to help her out, I would do it."
Just the facts on keratoconus
• Who gets keratoconus?
Researchers estimate the disease affects one in 2,000 people.
• Symptoms?
Subtle vision changes in early stages to bulging eyes in later stages.
• Are both eyes affected?
Yes, in about 90 percent of keratoconus cases. "
Intacs was first developed as an alternative for low prescription laser eye surgery. This was appealing at the time as it promised to be a reversble procedure if it did not work. From what I can understand it really did not take off as laser proved to be a better option. A few years back Intacs was first used to treat keratoconus with mixed results. The latest peer reviewed paper that has been published is:
Kanellopoulos AJ, Pe LH, Perry HD, Donnenfeld ED.
Modified intracorneal ring segment implantations (INTACS) for the management of moderate to advanced keratoconus: efficacy and complications.Cornea. 2006 Jan;25(1):29-33.
The conclusion was:
"The procedure appears to be effective in improving UCVA and BSCVA of patients with clinical keratoconus. In our small study group, however, there were significant (6/20) postoperative problems with regards to thinning and ring exposure."
Essentially what the take home message is that Intacs can be effective in allowing to get better vision from spectacles, which in itself is a great thing, but approximately 1/3 of the patients had significant complications 3 - 6 months later. I can guarantee that the group of ophthalmologists that have published this study are some of the best in the world.
The young lady in the article above that is having the hair cut fund raiser is hoping that this procedure will rid her of her keratoconus. I hope she has been advised accurately of the success rate of this technique.
We have just started using Intacs in Australia just recently. I am sure it will have a role in the management of keratoconus. At present I can see it helping patients with low levels of keratoconus or patients that cannot be fitted with contact lenses but do not want to have a corneal transplant. Stay tuned and I am sure more information will be coming out soon.
"Cutting hair for a worthy cause
Moxie hairdresser sets up fundraisers for a friend in need
By John C. Ensslin, Rocky Mountain News February 13, 2006
Erynn Simone looked across the room at Moxie Hair Co. in Denver, where a few feet away Talie Ayers, one of her childhood friends, was straightening a young woman's jet-black hair.
Simone, 22, could not see Ayers, nor the young woman.
That was why Ayers and six other hair stylists were working on a Sunday when the Capitol Hill hair salon normally would have been closed.
Simone is gradually losing her eyesight to keratoconus, an eye condition in which the normally dome- shaped cornea thins, causing a cone-like bulge of the cornea and blurred vision.
On Friday, Simone is scheduled to undergo a procedure to correct the condition. She will receive Intacs, which according to the National Keratoconus Foundation's Web site, are trademark prescription inserts approved by the Food and Drug Administration in July 2004.
Intacs are micro-thin, semi-circular plastic rings that are inserted into the mid-layer of the cornea, in an attempt to flatten it and improve vision.
The relatively new procedure will cost Simone about $7,000 and it is not approved by her medical insurance. So on Sunday, the hair stylists set to work, hoping to raise as much as they can toward the cost.
"Without the fundraiser, I probably wouldn't have the option of doing it. There's no way I would have the money," said Simone, who teaches environmental education in an after-school program at the Wild Bear Center for Nature Discovery in Nederland.
Ayers, who grew up with Simone in Three Rivers, Mich., had to convince her friend to let the hair salon do the fundraiser.
"I've just known her for so long," Ayers said. "If I could do anything to help her out, I would do it."
Just the facts on keratoconus
• Who gets keratoconus?
Researchers estimate the disease affects one in 2,000 people.
• Symptoms?
Subtle vision changes in early stages to bulging eyes in later stages.
• Are both eyes affected?
Yes, in about 90 percent of keratoconus cases. "
Intacs was first developed as an alternative for low prescription laser eye surgery. This was appealing at the time as it promised to be a reversble procedure if it did not work. From what I can understand it really did not take off as laser proved to be a better option. A few years back Intacs was first used to treat keratoconus with mixed results. The latest peer reviewed paper that has been published is:
Kanellopoulos AJ, Pe LH, Perry HD, Donnenfeld ED.
Modified intracorneal ring segment implantations (INTACS) for the management of moderate to advanced keratoconus: efficacy and complications.Cornea. 2006 Jan;25(1):29-33.
The conclusion was:
"The procedure appears to be effective in improving UCVA and BSCVA of patients with clinical keratoconus. In our small study group, however, there were significant (6/20) postoperative problems with regards to thinning and ring exposure."
Essentially what the take home message is that Intacs can be effective in allowing to get better vision from spectacles, which in itself is a great thing, but approximately 1/3 of the patients had significant complications 3 - 6 months later. I can guarantee that the group of ophthalmologists that have published this study are some of the best in the world.
The young lady in the article above that is having the hair cut fund raiser is hoping that this procedure will rid her of her keratoconus. I hope she has been advised accurately of the success rate of this technique.
We have just started using Intacs in Australia just recently. I am sure it will have a role in the management of keratoconus. At present I can see it helping patients with low levels of keratoconus or patients that cannot be fitted with contact lenses but do not want to have a corneal transplant. Stay tuned and I am sure more information will be coming out soon.
Introduction
Hi my name is Jim Kokkinakis. I am an optometrist in the CBD of Sydney and one of my specialties is a condition called keratoconus or conical cornea.
This condition is not that common ie it affects approximately 1/2000 of the general population. Over the years I have seen many hundreds of keratoconic patients, whereas a general optometrist will see approximately one keratoconic patient per year.
The main purpose of this blog is to raise the level of information on this very misunderstood condition and hopefully lower the level of concern that commonly is perpetuated by misinformation.
I invite you to regularly come back and I promise to keep updating and discuss the information that I post.
Keratoconus is NOT a blinding condition! It certainly can be very inconvenient to treat some times but the reality is that the overwhelming majority of people that exhibit this condition will continue life normally and be productive members of society.
This condition is not that common ie it affects approximately 1/2000 of the general population. Over the years I have seen many hundreds of keratoconic patients, whereas a general optometrist will see approximately one keratoconic patient per year.
The main purpose of this blog is to raise the level of information on this very misunderstood condition and hopefully lower the level of concern that commonly is perpetuated by misinformation.
I invite you to regularly come back and I promise to keep updating and discuss the information that I post.
Keratoconus is NOT a blinding condition! It certainly can be very inconvenient to treat some times but the reality is that the overwhelming majority of people that exhibit this condition will continue life normally and be productive members of society.
